Source: Mount Elizabeth
When exactly should you start checking for heart disease, and how does a doctor screen and diagnose a heart condition? Cardiologist Dr Paul Ong explains the details.
As the saying goes, early detection saves lives.
This rings true especially for heart disease, because discovering a heart condition early will allow a doctor to take the necessary steps to diagnose the exact issue and prevent the condition from worsening.
Screening for heart disease does not have to happen only when symptoms such as shortness of breath after a walk, or chest pain, show up. It should happen as part of a routine health screening, with many options conveniently available too.
Dr Paul Ong, cardiologist at Mount Elizabeth Novena Hospital, details some common heart screening options, the abnormalities he looks out for, and the investigative diagnostic procedures he may undertake to make an accurate diagnosis.
When should someone start considering screening for heart disease?

Men aged 40 and above, and women aged 50 and above, should start screening for heart disease. They should get screened even earlier if there are co-existing risk factors such as hypertension, diabetes, high cholesterol, a smoking habit, or family history of heart disease.
What are some common symptoms of a heart condition that people should look out for?
The most frequent complaint patients share is chest discomfort. Patients with heart disease typically complain about chest pain, and experience sensations such as a heavy weight ‘sitting on’ the chest. Other common complaints include breathlessness on exertion, heart palpitations, dizziness and even blacking out.
What are some of your commonly recommended heart screening options?

A thorough consultation with a doctor is really useful. Other investigations would often include blood tests to measure cholesterol and blood sugar levels. As part of the blood tests, liver and kidney functions and full blood count is also checked.
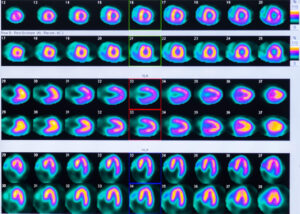
Specific investigations for the heart would include a resting ECG (electrocardiogram) and if required, an ultrasound scan of the heart (echocardiogram) and exercise treadmill tests may also be recommended. People with multiple risk factors, along with symptoms suggestive of a heart problem are frequently referred for a CT scan (computerised tomography) of the heart arteries.
What are some abnormalities you look out for during a screening?
It is important for me to know the medical history of my patients, and to look out for symptoms of heart disease so I can conduct the relevant investigations. Abnormal ECG and echocardiogram readings will certainly trigger more discussions and influence plans for either further investigations or follow ups.
What are the investigative procedures that you'd recommended to confirm a diagnosis?
A Holter ECG or ambulatory ECG allows the doctor to capture every heart beat over 1 – 7 days and can be useful to assess patients who experience frequent palpitations and dizziness.

An exercise treadmill ECG is often ordered to investigate symptoms of chest pain on exertion. The doctor will look at any new ECG changes during a high heart rate.
An echocardiogram is particularly helpful for people with a history of hypertension and those who experience shortness of breath on exertion. This is an indispensable test to investigate heart failure and heart valve disorders.
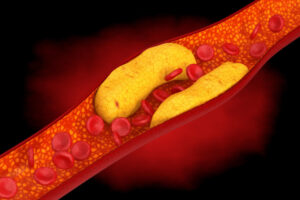
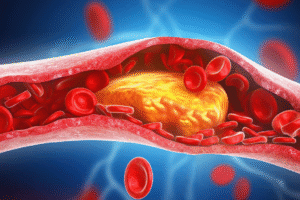
A CT scan of the heart which includes calcium score and coronary angiography can be very useful in assessing an individual’s risk of cardiac events, such as a heart attack. A relatively high calcium score of the heart artery will put a person at higher risk of cardiac events and thus warrant a more aggressive approach in controlling modifiable risk factors such as cholesterol and blood pressure. These risk factors can be managed with medication, a change of lifestyle and diet, or a combination of both.
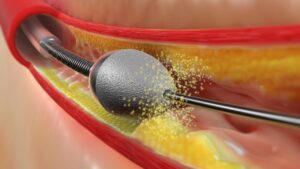
A CT coronary angiogram can detect if there are any obstructions in the heart arteries, where the obstruction is occurring, and how severe it is. Such a test allows for a more tailored discussion with our patients on how to manage and treat their heart disease. This may vary from simply optimising the medical therapy to planning for coronary angioplasty with balloon and stents or even coronary bypass surgery.
What are some common heart conditions that you often encounter in your practice?
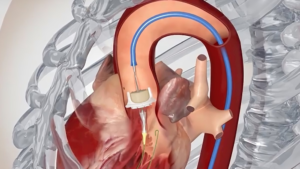
As an interventional cardiologist specialising in coronary artery disease, I see a lot of patients with blocked heart arteries presenting with chest pain. An invasive coronary angiogram done via the wrist artery (radial artery) is often done to get a clear picture of any artery blockage. Once the diagnosis is confirmed, it is often followed by inserting a balloon and stents to remove the obstruction in the vessel.
What happens if a screening yields normal results, yet does not explain a patient's symptoms, such as chest pain?
There are a small group of patients who come to me with classical symptoms of heart pain (angina) and often with abnormal exercise ECG. Yet, they may have normal CT coronary angiogram scans showing widely patent (unobstructed) heart vessels.
This group of patients may have Coronary Microvascular Disease (CMD). Although the coronary microvascular system is one of the main components of coronary circulation, its relevance has been underestimated for a long time as microvessels are invisible using current imaging techniques, and their function may be assessed only indirectly. Specifically, 50 – 65% of patients with angina with non-obstructive coronary artery disease are believed to have CMD.
Many of these patients were discharged from follow up as their conventional imaging tests were normal. They are then left frustrated without a firm diagnosis of their symptoms and often end up visiting many doctors across various specialties looking for a diagnosis and treatment. Worse still, many end up being admitted to hospital repeatedly with heart attacks.

There is now a new test using devices such as the coroventis physiological system to assess microvascular disease. It is carried out at the same time as an invasive coronary angiogram with a special pressure wire inserted into the coronary artery. The microvascular physiology is then measured with the thermodilution technique. The measured intramuscular resistance (IMR) will provide an objective assessment for CMD. In experienced hands, it usually takes an extra 10 – 15 minutes to perform the test during the coronary angiogram.
Patients with a normal coronary angiogram, and who also have CMD ruled out, can be reassured that they do not require further cardiovascular investigations and therapies. However, those with CMD benefit not just from having a confirmed diagnosis, but can receive tailored treatment to help manage their condition and improve their quality of life.